





Sickle cell disease (SCD) refers to a group of inherited blood disorders whose cause is strictly genetic. People who suffer from one of these disorders are born with an altered form of the HBB gene, which encodes for the β-globin subunit of the adult hemoglobin (HbA).
By around six months postnatal, a progressive switch from the intact fetal hemoglobin (HbF) to the altered HbA occurs, thus leading to a structural aberration in red blood cells (RBCs) and, therefore, functional changes of increasing severity in the entire body. The altered HbA, namely hemoglobin S (HbS), aggregates into rigid polymers within RBCs, causing these biological vehicles to acquire a sickle-like shape. As a result, fatigue and pain are the core somatic symptoms from which all physical and psychological constraints emerge.
Vasoocclusive crises (VOCs) represent the most severe issue physicians try hard to manage with pain relievers such as opioids. These recurrent painful crises usually compel patients to get hospitalized for urgent care, and repeated hospitalization disables them to normally perform their daily social activities, such as going to school and workplace, as their healthy counterparts do.
This early-age genetic condition has long been considered an absolutely somatic illness whose complications appear and get progressively more severe in almost a similar manner among patients. However, the relatively recent interest in the health-related quality of life (HRQoL) has changed the way scientists look at such chronic diseases of somatic origin. Yet there is currently consensus that a panoply of psychosocial factors plays a major role in modulating the prognosis of lifelong diseases such as SCD. In other words, patients have been shown to be very sensitive to the HRQoL factors they experience daily, and their life expectancy, which is a clinical term related to survival time, depends on whether these factors are favorable.
Our review article hypothesized that SCD has a psychosomatic component. This hypothesis is founded on observations suggesting that the psychosocial status of patients influences the onset and subsequent aggravation of somatic complaints. After analyzing a number of clinical studies that focus on patients’ HRQoL through questionnaire-based diagnoses, we noticed that a pathological cycle could take place. This cycle begins with the fact that patients develop anxiety and/or depressive disorders as their disease progresses.
Though these neuropsychiatric symptoms are prevalent in almost all chronic diseases, their severity in SCD appears to arise when patients realize that this health issue is untreatable, thus forcing them to deal with a psychosocial burden throughout their life. To do so, patients have been shown to acquire adaptive behavioral strategies that, inadvertently, make their condition more stressful. The cumulative stress is thought to interfere with the somatic complaints through a complex psychosomatic effect. It is, however, unknown when exactly this effect starts, even though the treating physicians can easily determine the onset of anxiety and/or depression and prescribe some drugs in case they feel it is quite necessary to prevent advanced mental disorders. Unfortunately, due to a complex interaction between physical, psychological, and social factors, medications are far from being able to solve the problem!
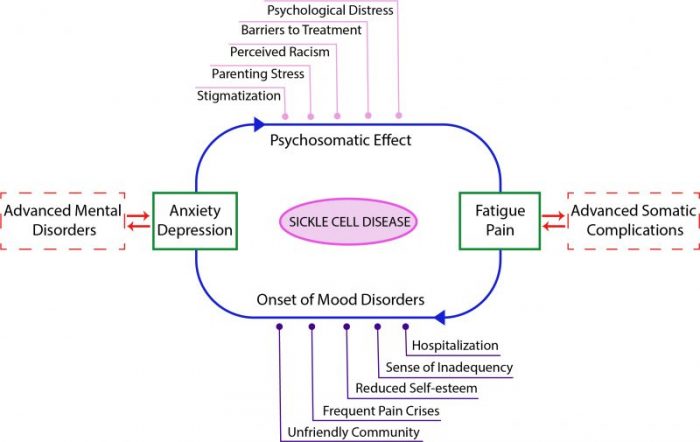
Image credit: Mohamed L. Toumi & Sameha Merzoug
The reviewed studies provided evidence that SCD est related to a high risk for life-threatening complications, such as stroke and heart attack, through a pathological mechanism that involves the emotional state of patients. All surrounding psychosocial signals patients perceive, including what is known as parenting stress, can cause mood disorders at any developmental stage, with those appearing in adulthood are found to be more serious and less controllable with anxiolytics/antidepressants.
For this reason, current medical efforts consider preventing the psychosomatic effect of SCD, or breaking it down once it has occurred, by cotreating somatic and neuropsychiatric complaints at the earliest. Otherwise, alternatives to such pharmacological interventions are behavioral and target the neuropsychiatric facet of the disease. A frequently used procedure with patients is the cognitive behavioral therapy (CBT), which has been reported to alleviate their stress, increase their self-esteem within society, and teach them how to deal with their illness, particularly on crisis pain days, in the most appropriate way possible.
Based on the reviewed clinical studies, we can state that SCD is more complex than previously thought due to the high number of interfering factors. Physicians should give a particular attention to the quality of life determinants in each patient while controlling for the onset of anxiety and/or depression. Pharmacological cotreatments are recommended as long as they help manage painful crises and mood disorders without significant side effects. Otherwise, the application of CBT techniques appears to be effective in decreasing the overall severity of complications.
These findings are described in the article entitled Does sickle cell disease have a psychosomatic component? A particular focus on anxiety and depression, recently published in the journal Life Sciences. This work was conducted by Mohamed Lamine Toumi and Sameha Merzoug from the University of Chadli Bendjedid, and Mohamed Rachid Boulassel from Sultan Qaboos University.
Related Posts
 Important Strategies To Help Healthcare Providers Support Patients With Diabetes
Important Strategies To Help Healthcare Providers Support Patients With Diabetes Studying The Link Between Increased BMI And Late-Onset Preeclampsia In Pregnant Women
Studying The Link Between Increased BMI And Late-Onset Preeclampsia In Pregnant Women A Bacterial Cell Imaging Method Using CRISPR And Microfluidics
A Bacterial Cell Imaging Method Using CRISPR And Microfluidics B. infantis Reduces Key Markers Of Intestinal Inflammation In Infants
B. infantis Reduces Key Markers Of Intestinal Inflammation In Infants Epigenetic Changes In Multiple Sclerosis – Studied In Twins
Epigenetic Changes In Multiple Sclerosis – Studied In Twins Did You Know Math Can Help Us Learn How Diseases Work?
Did You Know Math Can Help Us Learn How Diseases Work?