





Hematopoietic cell transplantation (HCT – formerly termed “bone marrow transplantation”) is an established treatment for patients with life-threatening hematological and non-hematological diseases, including acute and chronic leukemias, myelodysplastic syndromes, lymphomas, multiple myeloma, aplastic anemia, immune disorders, and congenital disorders of metabolism, and may result in remission or cure in a proportion of cases.
HCT involves the administration of high-dose chemotherapy to ablate cancerous cells in the bone marrow or elsewhere in a patient, followed by an infusion of hematopoietic cells previously collected from an HLA-matched related or unrelated donor (allogeneic HCT), or the patient themselves (autologous HCT), to repopulate the patient’s bone marrow.
Numbers of HCT performed worldwide is reported to have risen steadily in recent years. In addition, numbers of HCT survivors continue to increase. In Australia and New Zealand (A&NZ), total annual numbers of autologous and allogeneic HCT increased from 1,359 in 2005 to 1,736 in 2013 and 1,966 in 2015, a 2005-15 increase of 45%.
The Australasian Bone Marrow Transplant Recipient Registry (ABMTRR) commenced collecting data Australia-wide in 1992; transplant centers in New Zealand have contributed since 1998. By the conclusion of 2013, the ABMTRR had accrued more than 25,000 transplant records from 50 participating centers. Ownership of ABMTRR data is shared by the contributing institutions, which are collectively represented by the Bone Marrow Transplant Society of Australia and New Zealand (BMTSANZ). The ABMTRR has a high compliance rate, with all known HCT centers in A&NZ contributing annually.
A study carried out in the USA in 2008 predicted an increased need for HCT physicians and a possible shortage in future years. A detailed study published in 2011 reported that numbers of allogeneic HCT in the USA had increased by 29.9% in the period 2005 to 2009.
This study aimed to collect and analyze details on transplant physicians and centers in A&NZ, report on relevant indicators of capacity and output measures and compare results with international experience, to assist in future management and planning.
Method
All centers performing allogeneic and/or autologous HCT that report to the ABMTRR were invited to participate in this study. Every center that consented to participate was sent a data entry spreadsheet asking for demographic and workforce details of physicians who participate in the primary care of HCT patients at the center, plus questions on bed capacity and numbers of junior medical staff. Responses were collected from participating centers between October 2015 and August 2016. Centers were classified as performing either “Autologous only” or “Autologous and allogeneic” HCT — there were no “Allogeneic only” centers.
Results
From the 46 centers that were invited to participate, completed data were received from 37 (80%). Of the responding centers, 19 performed both allografts and autografts, representing a total of 633 allografts and 607 autografts in 2015. A further 18 centers performed autografts only, representing a total of 512 autografts in 2015. Results were received from 31 adult and 6 pediatric centers; 33 were located in Australia and 4 in New Zealand.
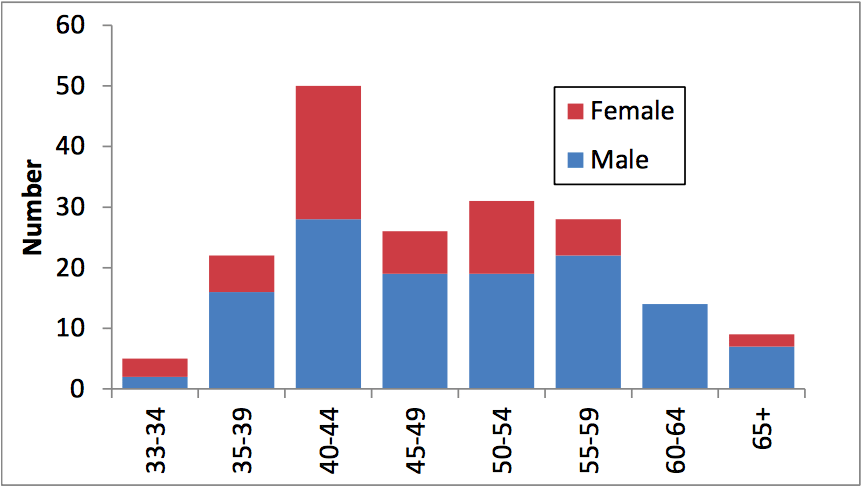
Figure 1. Age and sex distribution of HCT physicians (Republished with permission from Elsevier)
Among 185 HCT physicians surveyed, 127 (69%) were male; the median age was 48 with a range of 33 to 72, 97 (52%) had prior experience in overseas centers, and 79 (43%) had postgraduate qualifications other than specialist training.
HCT physicians spent their time on a variety of tasks, including caring for HCT patients, research, administration, research and general hematology duties. For HCT physicians working at “allo plus auto” centers, the average proportion of time spent on HCT-related duties was 43.9%, while for physicians working at “auto only” centers it was 18.9%.
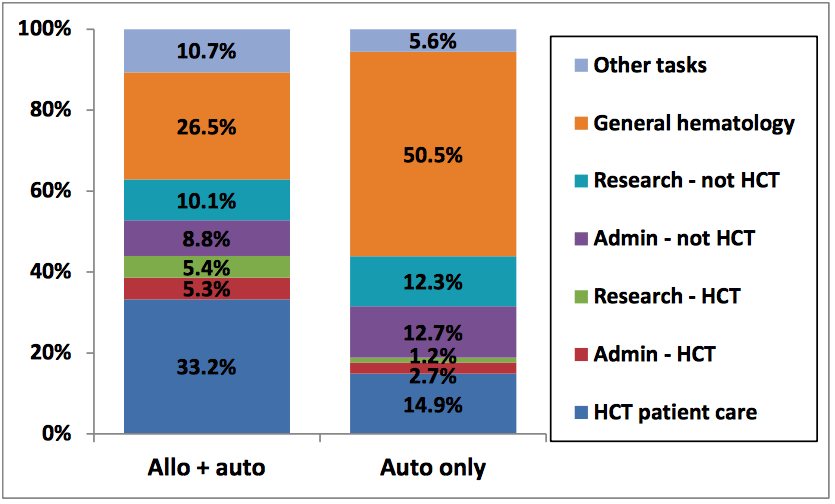
Figure 2. Proportion of HCT physician time spent on tasks, by center type (Republished with permission from Elsevier)
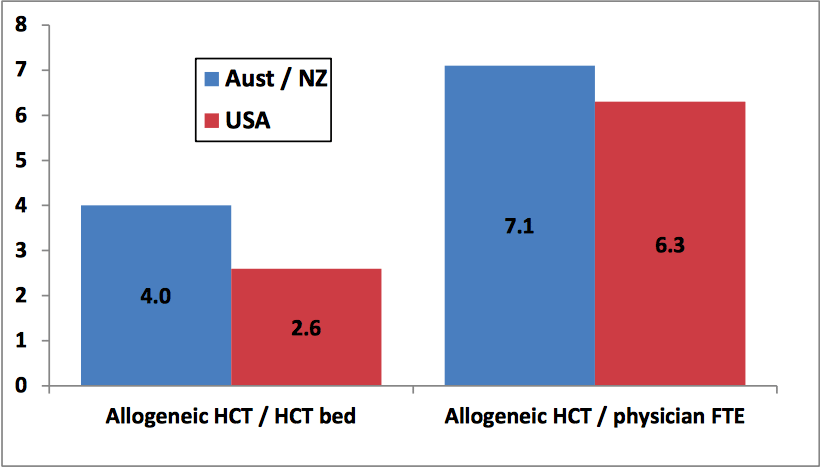
Figure 3. Indicators of allogeneic HCT activity: comparison of A&NZ allo + auto centers (2015) and US allo centers (2009) (Republished with permission from Elsevier)
We can make cautious comparisons between HCT administration in A&NZ and the USA. Analysis indicated that A&NZ “allo plus auto” centers were slightly higher than USA “allo” centers in terms of both HCT bed utilization and allogeneic HCT numbers per HCT physician.
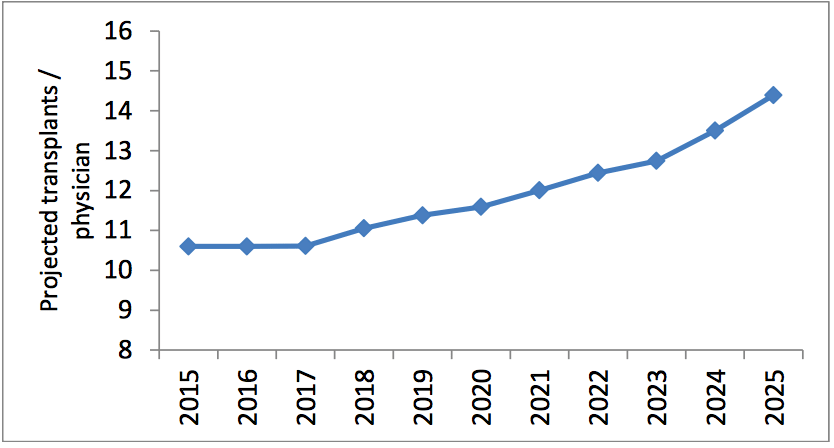
Figure 4. Projected annual numbers of HCT per physician FTE, A&NZ, 2015 – 2025 (Republished with permission from Elsevier)
The steady increase in HCT activity in A&NZ in recent years can be attributed to a greater availability of potential allogeneic donors, improved HCT techniques enabling HCT physicians to transplant older and more extensively pre-treated patients, a widening of diseases which may be treated by HCT (e.g. autoimmune diseases) and an ageing population which mediates an increase in the incidence of diseases where HCT is recommended as treatment. If HCT numbers in A&NZ continue to increase at a steady rate, without a commensurate increase in HCT physician recruitment and training or an increased allocation of HCT physician time to patient care, an impending workforce shortage of trained HCT physicians may impact the ability to deliver optimum care to the large number of patients envisaged to require this complex treatment over the next decade.
These findings are described in the article entitled Activity and Capacity Profile of Transplant Physicians and Centers in Australia and New Zealand, recently published in the journal Biology of Blood and Marrow Transplantation.
This work was conducted by Ian Nivison-Smith, Samuel Milliken, Anthony Dodds, David Ma, and Leonie Wilcox from St. Vincent’s Hospital, David Gottlieb and John Kwan from Westmead Hospital, Peter J. Shaw from Children’s Hospital Westmead, Steven Tran from the Australasian Bone Marrow Transplant Recipient Registry, and Jeffrey Szer from Royal Melbourne Hospital.
For more information on this research please see: Ian Nivison-Smith, Samuel Milliken, Anthony J Dodds, David Gottlieb, John Kwan, David DF Ma, Peter J Shaw, Steven Tran, Leonie Wilcox, Jeff Szer. Activity and Capacity Profile of Transplant Physicians and Centers in Australia and New Zealand. Biology of Blood and Marrow Transplantation, January 2018, 24:169-174.
Related Posts
 Important Strategies To Help Healthcare Providers Support Patients With Diabetes
Important Strategies To Help Healthcare Providers Support Patients With Diabetes Studying The Link Between Increased BMI And Late-Onset Preeclampsia In Pregnant Women
Studying The Link Between Increased BMI And Late-Onset Preeclampsia In Pregnant Women A Bacterial Cell Imaging Method Using CRISPR And Microfluidics
A Bacterial Cell Imaging Method Using CRISPR And Microfluidics B. infantis Reduces Key Markers Of Intestinal Inflammation In Infants
B. infantis Reduces Key Markers Of Intestinal Inflammation In Infants Epigenetic Changes In Multiple Sclerosis – Studied In Twins
Epigenetic Changes In Multiple Sclerosis – Studied In Twins Did You Know Math Can Help Us Learn How Diseases Work?
Did You Know Math Can Help Us Learn How Diseases Work?